
HISTORY
Any plastic surgeon that performs breast augmentation with implants will inevitably deal with symptoms, complaints, problems and the need for revision. Period. I am completely sensitive to why patients want to look and feel normal again. Breast Augmentation Revision (BAR) is now a specialty unto itself and rapidly evolving and improving in the techniques, the technology, the implants and the prevention of recurrence. Some surgeons, like myself, have the years of experience, continued learning and special expertise to best be able to address the broad spectrum of BAR problems and cure these with a very high degree of predictability. The silicone implants first invented and used in 1963 have now evolved to the fifth, maybe sixth generation of improvement in silicone filler composition (from liquid to gel to semisolid-cohesive), implant shell thickness and texture, different shapes and dimensions and more. The techniques of dealing with implant space, the collagen capsule, prevention of contracture and more have dramatically changed and improved. Fortunately, all the symptoms and conditions patients complain of now do lend themselves to a very predictable improvement and cure.
INDICATIONS
What patient complaints and concerns years ago began as cosmetic dissatisfaction or hardening of the breast and capsular contracture now have evolved to concerns with even its mildest form of dissatisfaction with size (want to be bigger or smaller), asymmetry, breast upper pole bulging or asymmetry, lack of centralization of the nipple-areolar complex (NAC), different degrees of pain, and more recently and importantly, to now what we recognize as Breast Implant Illness (BII – read more here about BII) and the symptoms that might be associated with silicone in breast implants. So, every plastic surgeon must have experience with this and knowledge of the full spectrum of the history of breast implants, the symptoms, BEST options, alternatives and treatments, and yes, the cures. Dr Romano has a long experience with successful BAR, and where indicated, removal of implants and the options. This includes vast experience with saline, silicone implants; shapes (anatomic and round), dimensions, textured and smooth. He has always put patients and their expectations first, educates patients, performs to the highest technical and professional standards, has never had any infections or tragedies or lawsuits, and consistent excellent results.
Patients seek revision or removal of breast implants for any number of single or combined reasons:
COSMETIC
- Size. Too big or too small
- Deformity. Upper pole bulging, bottoming out, too much or little cleavage. Rippling, wrinkles, lack of roundness. Movement or displacement of implants into armpit, too low, too high or across the midline (“uniboob”).
- Asymmetry. One too big or too small or just different shape or look.
- Hardening. Capsular contracture. This is graded as levels I-IV from just noticeable to hard and severe.
FUNCTIONAL
- Pain. This can be from the capsular contracture or even numbness
- Constitutional symptoms. This is Breast Implant Illness (BII) and can range from mild to severe and there is a spectrum of symptoms from most commonly fatigue, brain fog and joint pains up to loss of libido, hair loss and more.
PERSONAL
- When patients tell me “I am over implants and just want them removed” and there needs to be no further discussion, and I agree and offer options.
EVALUATION
Dr Romano will review with you carefully and in great detail your current issues and expectations, what your anatomy is now, what procedures you have had done, and what your body and anatomy will safely allow to provide safe and predictable results. This will involve providing as much information with a special breast revision intake form, a long and detailed educational consultation and exam, review of previous operative reports when available, and highly customized formulation of a plan with you. There may be a role for some blood testing and imaging such as mammogram and MRI, but only if indicated. Dr Romano will review carefully any BII or symptoms you may have and offer a plan to, as is mostly the case, cure these symptoms.
SURGERY OVERVIEW
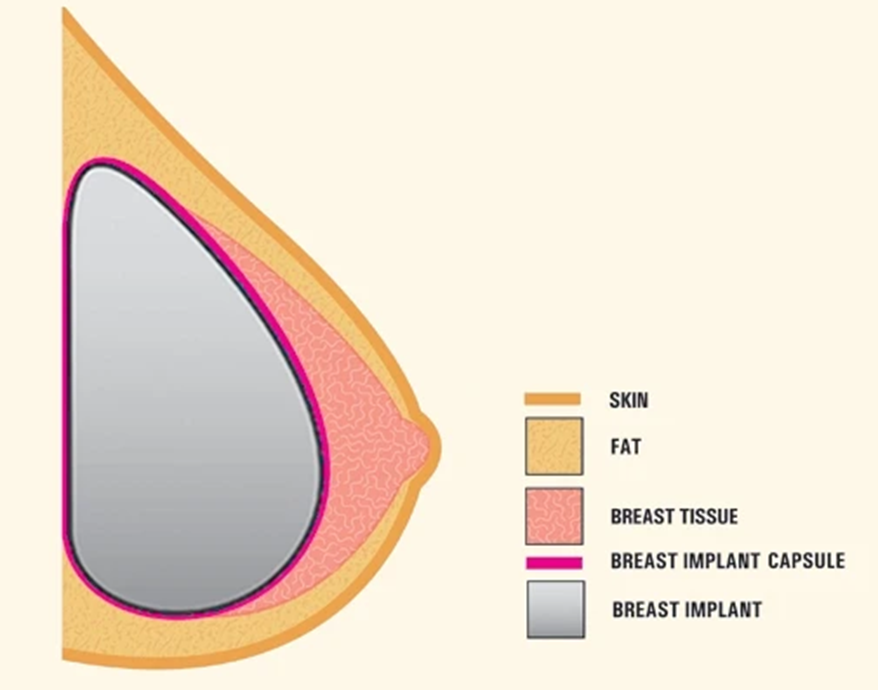
Once it is determined what is the best procedure, it always is by the nature of things, highly customized and detailed. Be advised there is a broad spectrum of what surgeons offer and are comfortable with and will propose to you and this may not be the state of the art. Dr Romano will be completely detailed and thoroughly educate you about the current best option and best procedure that you both mutually agree upon and will best address your expectations, anatomy and a cure. To start with, the basics of the procedure ultimately boil down to how your surgeon will deal with the STATUS and TREATMENT of the breast implant capsule. This guides the whole of the surgical plan. See in the diagram below the dark/purple rim of collagen tissue that forms around every implant. If this is normal, then only suturing or exchanging implants or removing implants is done, as indicated. If, however, the capsule is irritated or has bacteria (biofilm – read Dr Romano’s paper on this) impregnated in the capsule then it is hard and tight and distorts the implant. In this case, I believe it needs to be totally or near totally removed (total capsulectomy). This removes the infected-diseased collagen tissue and the encapsulated bacteria, and prevents recurrence. In this category of procedure, once the capsule is removed then the breast space is adjusted by enlarging if it is too tight, or closing with sutures if it is too big, again, as indicated. Once this is done Dr Romano next inserts a temporary implant, sits up the patient in the operating room and with full effect of gravity, makes sure the size is just right, there is evenness and symmetry, and the breast looks natural with the nipple in the middle, smooth on top, and rounding on the bottom, not too wide, and just right cleavage. Once all of this is as perfect as your body will allow, you are laid flat, the temporary implants are removed, and the next step done is very important. This is where preoperatively I insist on implantation of a product called Strattice that is a dermal matrix material and 95% of the time will prevent recurrence of the contracture. It is a sheet material that wraps around the implant and prevents abnormal thick scar tissue capsule formation. The incisions are closed with all hidden dissolvable stitches. Since the surgery is started by giving a Novocaine injection all around the breasts, you do not need as deep a general anesthetic and you wake up numb but not in pain, no nausea, and just slightly drowsy. This anesthetic routine and Novocaine serves to break the pain cycle and means recovery is comfortable and almost painless.
See collagen capsule depiction and anatomy as the dark/purple around the implant:
SURGERY SUMMARY
As a summary, the surgical basic elements and options are as follows but may be some variations:
- Virtually always use your original incisions and never a need to make large or new or unsightly incisions.
- Outpatient surgery with board certified anesthesiologist with special expertise in cosmetic surgery and works with Dr Romano all the time.
- Capsule not contracted: remove implants and replace new or leave out per patient
- Capsule not contracted but breast shape distorted: remove implants and put in stitches to correct deformity and put in new implants
- Capsule contracted: remove implants make cuts in capsule to release tightness (capsulotomies) and put in new implants. Dr Romano NEVER does this with capsular contracture since the whole abnormal capsule needs to be removed or it will recur.
- Capsule contracted: remove implants, remove entire capsule (complete capsulectomy). Correct capsule space with internal sutures. Put in Strattice (Dr Romano ALWAYS does this) and put in new implants. Keller funnel and lots of antibiotics.
- Always send the capsules to the pathology department to study and make sure there are no abnormal growths. This is VERY rare, and I have never had this in a patient.
- Use the Keller funnel to sterilely insert the implant and plenty of strong antibiotics in the breast space and IV.
- Dr Romano does not perform breast lifting at the same time as this always requires extensive external (boat anchor or lollipop) incisions. These always interrupt the blood supply and, so, adds great risk to healing. This is mostly never needed but can always be done at a second stage if required.
- Be prepared to do fat grafting to help shape or add padding to the breast if safe, or this can be done at a second procedure, especially if the patient wants implants totally removed.
RECOVERY
Surgery is done in an outpatient fully accredited and very safe and private surgery center. He works with a board-certified anesthesiologist specialist in cosmetic surgery procedures. You go to sleep quickly and gently, and he then injects Novocaine all around the breast to totally numb up the area. With this done, the anesthesia doctor can then reduce your dose to the bare minimum to keep you totally asleep. The surgery is safe and predictable. You wake up numb but in no pain and this means you will have no pain or much reduced pain in recovery. You will be very alert and virtually no nausea or vomiting. Immediately after surgery, you will see your results and it just gets better with time. All the stitches are dissolvable, and the recovery is rapid; you can return to work in several days and to some physical exercise within the first week. Dr Romano will teach you how to massage, use prophylactic antibiotics and more to prevent recurrence.
For more information contact the office info@sfplasticsurgery.org or 415 981 3911.
Here is the link to the website Breast Augmentation Revision section if you have not already viewed it.
